– The US Healthcare System: Most Expensive Yet Worst In The Developed World (Zerohedge, June 22, 2014):
One month ago we showed that when it comes to the cost of basic (and not so basic) health insurance, the US is by far the most expensive country in the world and certainly among its “wealthy-nation”peers (in a world in which indebtedness is somehow equivalent to wealth), which in the context of the irreversible socialization of American healthcare, was in line with expectations.

It would be logical then to think that as a result of this premium – the biggest in the world – the quality of the healthcare offered in the US among the best, if not the best, in the world. Unfortunately, that would be wrong and, in fact, the reality is the complete opposite: as a recent study by the Commonweath Fund, looking at how the US healthcare system compares internationally, finds, “the U.S. fails to achieve better health outcomes than the other countries, and as shown in the earlier editions, the U.S. is last or near last on dimensions of access, efficiency, and equity.” In other words: most expensive, yet worst in the developed world.

From the report:
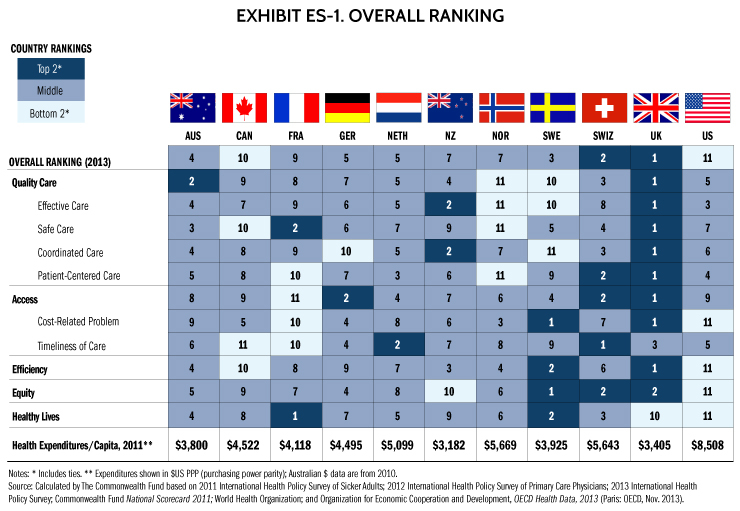
The United States health care system is the most expensive in the world, but this report and prior editions consistently show the U.S. underperforms relative to other countries on most dimensions of performance. Among the 11 nations studied in this report—Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, the United Kingdom, and the United States—the U.S. ranks last, as it did in the 2010, 2007, 2006, and 2004 editions of Mirror, Mirror. Most troubling, the U.S. fails to achieve better health outcomes than the other countries, and as shown in the earlier editions, the U.S. is last or near last on dimensions of access, efficiency, and equity. In this edition of Mirror, Mirror, the United Kingdom ranks first, followed closely by Switzerland (Exhibit ES-1).
Expanding from the seven countries included in 2010, the 2014 edition includes data from 11 countries. It incorporates patients’ and physicians’ survey results on care experiences and ratings on various dimensions of care. It includes information from the most recent three Commonwealth Fund international surveys of patients and primary care physicians about medical practices and views of their countries’ health systems (2011–2013). It also includes information on health care outcomes featured in The Commonwealth Fund’s most recent (2011) national health system scorecard, and from the World Health Organization (WHO) and the Organization for Economic Cooperation and Development (OECD).
The most notable way the U.S. differs from other industrialized countries is the absence of universal health insurance coverage. Other nations ensure the accessibility of care through universal health systems and through better ties between patients and the physician practices that serve as their medical homes. The Affordable Care Act is increasing the number of Americans with coverage and improving access to care, though the data in this report are from years prior to the full implementation of the law. Thus, it is not surprising that the U.S. underperforms on measures of access and equity between populations with above- average and below-average incomes.
The U.S. also ranks behind most countries on many measures of health outcomes, quality, and efficiency. U.S. physicians face particular difficulties receiving timely information, coordinating care, and dealing with administrative hassles. Other countries have led in the adoption of modern health information systems, but U.S. physicians and hospitals are catching up as they respond to significant financial incentives to adopt and make meaningful use of health information technology systems. Additional provisions in the Affordable Care Act will further encourage the efficient organization and delivery of health care, as well as investment in important preventive and population health measures.
For all countries, responses indicate room for improvement. Yet, the other 10 countries spend considerably less on health care per person and as a percent of gross domestic product than does the United States. These findings indicate that, from the perspectives of both physicians and patients, the U.S. health care system could do much better in achieving value for the nation’s substantial investment in health.
Major Findings
- Quality: The indicators of quality were grouped into four categories: effective care, safe care, coordinated care, and patient-centered care. Compared with the other 10 countries, the U.S. fares best on provision and receipt of preventive and patient-centered care. While there has been some improvement in recent years, lower scores on safe and coordinated care pull the overall U.S. quality score down. Continued adoption of health information technology should enhance the ability of U.S. physicians to identify, monitor, and coordinate care for their patients, particularly those with chronic conditions.
- Access: Not surprisingly—given the absence of universal coverage—people in the U.S. go without needed health care because of cost more often than people do in the other countries. Americans were the most likely to say they had access problems related to cost. Patients in the U.S. have rapid access to specialized health care services; however, they are less likely to report rapid access to primary care than people in leading countries in the study. In other countries, like Canada, patients have little to no financial burden, but experience wait times for such specialized services. There is a frequent misperception that trade-offs between universal coverage and timely access to specialized services are inevitable; however, the Netherlands, U.K., and Germany provide universal coverage with low out-of-pocket costs while maintaining quick access to specialty services.
- Efficiency: On indicators of efficiency, the U.S. ranks last among the 11 countries, with the U.K. and Sweden ranking first and second, respectively. The U.S. has poor performance on measures of national health expenditures and administrative costs as well as on measures of administrative hassles, avoidable emergency room use, and duplicative medical testing. Sicker survey respondents in the U.K. and France are less likely to visit the emergency room for a condition that could have been treated by a regular doctor, had one been available.
- Equity: The U.S. ranks a clear last on measures of equity. Americans with below-average incomes were much more likely than their counterparts in other countries to report not visiting a physician when sick; not getting a recommended test, treatment, or follow-up care; or not filling a prescription or skipping doses when needed because of costs. On each of these indicators, one-third or more lower-income adults in the U.S. said they went without needed care because of costs in the past year.
- Healthy lives: The U.S. ranks last overall with poor scores on all three indicators of healthy lives—mortality amenable to medical care, infant mortality, and healthy life expectancy at age 60. The U.S. and U.K. had much higher death rates in 2007 from conditions amenable to medical care than some of the other countries, e.g., rates 25 percent to 50 percent higher than Australia and Sweden. Overall, France, Sweden, and Switzerland rank highest on healthy lives.
Summary
The U.S. ranks last of 11 nations overall. Findings in this report confirm many of those in the earlier four editions of Mirror, Mirror, with the U.S. still ranking last on indicators of efficiency, equity, and outcomes. The U.K. continues to demonstrate strong performance and ranked first overall, though lagging notably on health outcomes. Switzerland, which was included for the first time in this edition, ranked second overall. In the subcategories, the U.S. ranks higher on preventive care, and is strong on waiting times for specialist care, but weak on access to needed services and ability to obtain prompt attention from primary care physicians. Any attempt to assess the relative performance of countries has inherent limitations. These rankings summarize evidence on measures of high performance based on national mortality data and the perceptions and experiences of patients and physicians. They do not capture important dimensions of effectiveness or efficiency that might be obtained from medical records or administrative data. Patients’ and physicians’ assessments might be affected by their experiences and expectations, which could differ by country and culture.
Disparities in access to services signal the need to expand insurance to cover the uninsured and to ensure that all Americans have an accessible medical home. Under the Affordable Care Act, low- to moderate-income families are now eligible for financial assistance in obtaining coverage. Meanwhile, the U.S. has significantly accelerated the adoption of health information technology following the enactment of the American Recovery and Reinvestment Act, and is beginning to close the gap with other countries that have led on adoption of health information technology. Significant incentives now encourage U.S. providers to utilize integrated medical records and information systems that are accessible to providers and patients. Those efforts will likely help clinicians deliver more effective and efficient care.
Many U.S. hospitals and health systems are dedicated to improving the process of care to achieve better safety and quality, but the U.S. can also learn from innovations in other countries—including public reporting of quality data, payment systems that reward high-quality care, and a team approach to management of chronic conditions. Based on these patient and physician reports, and with the enactment of health reform, the United States should be able to make significant strides in improving the delivery, coordination, and equity of the health care system in coming years.
* * *
It should, although if the government is in charge of it, as it now appears to be, it won’t.
No wallet left behind. Automatic 12% profit every year. Now they got obamacare to force the victims to buy it.